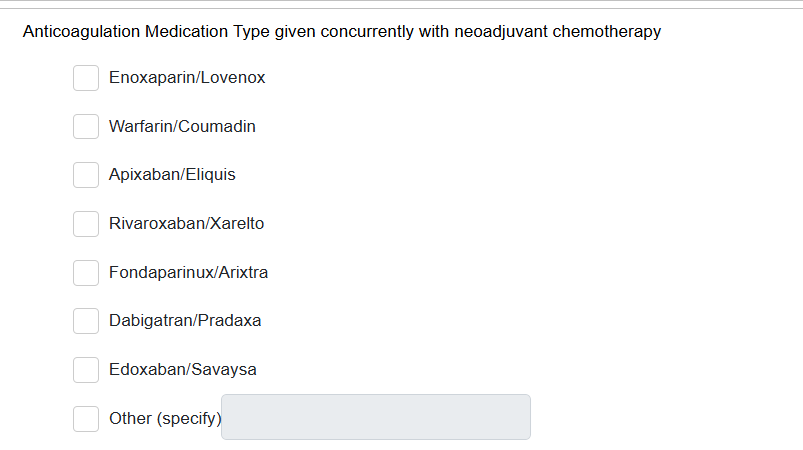
For GYN cases only. Indicate if the patient was prescribed any of the anticoagulation medications listed in the help text within 30 days of starting neoadjuvant chemotherapy.
Anticoagulation medications include LMWH/low molecular weight heparin,Warfarin/Coumadin, Apixaban/Eliquis, Rivaroxaban/Xarelto, Fondaparinux/Arixtra,Dabigatran/Pradaxa, and Edoxaban/Savaysa. “Concurrently” is defined as +/-30 days from neoadjuvant therapy start date